
Fungal Pharmacy
What Medicine Profits From Yet Won't Acknowledge In Your Environment

Right now, somewhere in the United States, a physician is writing a prescription for a drug that inhibits an enzyme involved in cholesterol synthesis. That same physician may have a patient sitting across from them with inexplicably dysregulated cholesterol who has been living in a water damaged building for two years. The physician will not connect those two facts — not because the connection doesn’t exist, but because no one ever taught them to look for or understand it.
The active ingredient in that prescription traces its origin directly to a mold. The mechanism it exploits — blocking a specific enzymatic step in cholesterol production — is the same mechanism the mold evolved as a competitive weapon against neighboring organisms. Medicine isolated that weapon, purified it and put it in a pill. And then, somehow, drew a hard line between what that molecule does in a controlled pharmaceutical context and what the organisms naturally producing it might do when they colonize the walls of a home.
This is the chasm and it is a wide one.
To be clear from the outset, the problem here is not that medicine uses fungal metabolites. Penicillin was a revelation and has saved millions of lives. Cyclosporine made organ transplantation survivable. The pharmaceutical exploitation of fungal chemistry is one of the great achievements of modern medicine and nothing in this article argues otherwise.
The problem is this: medicine possesses detailed, peer reviewed, in vivo (in the body, not the petri dish) knowledge of what specific fungal metabolites do inside the human body. It has published that knowledge, built industries on it and written prescribing guidelines around it. Yet when a patient presents with symptoms consistent with those same mechanisms — immune suppression, cholesterol dysregulation, neurological disruption, protein synthesis abnormalities — following documented exposure to the organisms that produce those same metabolites in their home or workplace, the clinical response is overwhelmingly disappointing and often outright dismissive. Moreover, there seems to be no curiosity in exploring a connection that, at least to me, seems undeniable based on what we already know from pharmacodynamics of the same or analogous compounds.
The irony compounds when you understand the scale. A pharmaceutical dose is usually measured in milligrams, administered once daily and metabolized on a defined schedule well elucidated via pharmacokinetic and pharmacodynamics studies done prior to drug release and approval. A mold colony the size of a dinner plate, living inside a wall cavity or beneath a bathroom floor, produces secondary metabolites, including mycotoxins, across a surface that grows larger over time if the conditions are right. The daily exposure model is the same. The concentration and route are different. Yet one is medicine and the other is dismissed as an impossibility.
The medical establishment at large disregards mold toxicity while it acknowledges drug toxicity of the same originating compound.
There is one more layer that gets almost no attention in clinical settings. When mold and bacteria coexist in a confined environment, as they always do in water damaged buildings, are not coexisting peacefully. They are at war. Both deploying chemical defense molecules to suppress and eliminate the competition. How do we know this from a scientific standpoint? The very breakthrough that opened fungal pharmacology to the world: penicillin.
Penicillin was famously discovered because Penicillium notatum in a petri dish had killed the bacterial colonies surrounding it. That was a contained observation in a laboratory setting. To date, no one has seriously applied that framework to microbial building biology — to what happens when competing colonies of mold and bacteria are simultaneously producing defensive metabolites inside the confined air space of a home that an occupant is breathing continuously.
And finally: the dose makes the poison, but biology is not uniform. Some physiologies handle medications at standard doses without incident; others experience significant adverse effects at fractions of the same dose. The same is true of mold exposure. Individual variation in detoxification capacity, immune competence and genetic susceptibility means that two people can occupy the same building and have dramatically different outcomes. This does not mean one of them is imagining it and furthermore this does not mean environmental medicine and toxicologists should discount this type of exposure.
Fungal Entry Into Pharmacology
In September 1928, Alexander Fleming returned from vacation to his laboratory at St. Mary’s Hospital in London. A petri dish he’d left on the bench had been contaminated by a mold — Penicillium notatum — and everywhere the mold grew, the bacteria he was studying were dead.
Fleming understood fairly quickly what he was looking at: a living organism producing a chemical potent enough to kill bacteria. One that could, he suspected, be translated into a treatment for human infection. He published his observations in 1929. The world took another decade to notice.
By 1943, penicillin was in mass production. By 1945, Fleming shared the Nobel Prize. By the mid-twentieth century, medicine had grasped a principle that would reshape pharmacology forever: fungi are master chemists and their metabolites are biologically active in ways medicine can exploit.
What followed was not one discovery but dozens.
Fungal Pharmacopoeia: What Your Doctor Likely Doesn’t Even Know
Most people know about penicillin and its origin. Very few people, including doctors, know about the other drug classes that rely on fungal metabolites as their active ingredients.
Some examples: the cephalosporins — antibiotics now prescribed hundreds of millions of times per year — were isolated from a fungus collected from a Sardinian sewage outfall in 1948. Griseofulvin, used to treat fungal nail infections, comes from Penicillium griseofulvum. Fusidic acid, used against MRSA, comes from Fusidium coccineum.
And then there are the big ones. The ones with proven mechanisms of action (MOAs) — and profit margins.
Cyclosporine was discovered in 1972 in a Norwegian soil sample. The organism was Tolypocladium inflatum. The compound it produced inhibits a specific immune pathway — calcineurin phosphatase — that T-cells depend on to activate. When the FDA approved it in 1983, cyclosporine transformed organ transplantation. Before it, transplant and graft survival rates were low. After it, kidney, heart, liver and lung transplants became routine. It works because a soil fungus evolved a chemical weapon that, when given to humans, shuts down the T-cell response and prevents rejection of a foreign tissue.
Fingolimod (Gilenya), approved for multiple sclerosis in 2010, was derived from myriocin — a metabolite produced by an insect killing fungus called Isaria sinclairii. It works by trapping lymphocytes inside lymph nodes so they cannot attack myelin and cause the hallmark demyelination seen in MS.
Ergot alkaloids — from Claviceps purpurea, the same fungus responsible for medieval outbreaks of gangrenous madness called St. Anthony’s Fire — gave us ergotamine for migraines, bromocriptine for Parkinson’s disease and methylergonovine for postpartum hemorrhage. Albert Hofmann’s synthesis of LSD in 1938 was a direct result of ergot alkaloid research. These drugs work because ergot alkaloids act on alpha-adrenergic, dopaminergic and serotonergic receptors. (Makes me think about the “madness” I felt in my townhouse.)
Fungi, then, are a foundation of modern pharmacology. They produce molecules that alter human biology in measurable, reproducible, clinically significant ways and we have been deliberately mining them for over a century.
So why does it seem we are deliberately discounting them in other applications?
In other words, the same medical establishment that dismisses mold toxicity as unproven has built an entire regulatory infrastructure around the toxicity of the drugs derived from it. Every fungal sourced pharmaceutical on the market carries a documented adverse effect profile. Cyclosporine — the soil fungus immunosuppressant — is nephrotoxic, neurotoxic and carries a black box warning for increased risk of malignancy and serious infection. Mycophenolate carries a black box warning for those same risks, plus teratogenicity severe enough to require pregnancy prevention protocols. Statins are associated with myopathy, rhabdomyolysis and hepatotoxicity. The FDA maintains MedWatch, an entire adverse event reporting system, precisely because drug toxicity is real, dose dependent and requires ongoing surveillance. Medicine does not question whether fungal metabolites can cause harm inside the human body when taken as a pill or infusion. It has codified, labeled and regulated that harm in exhaustive detail. It simply refuses to extend that same logic one step further — to the organisms producing those same metabolites in an uncontrolled indoor environment.
Statins: When a Scientist Went Looking in Fungi on Purpose
Did you know the most profitable drug class in the world, statins, come from fungus?
The global statin market generates approximately $16 - 37 billion per year. Atorvastatin (Lipitor) is the best selling pharmaceutical in history with over $150 billion in cumulative sales.
Read the American Scientist Article Here | Statins: From Fungus to Pharma
In 1968, a Japanese biochemist named Akira Endo took a fellowship at Albert Einstein College of Medicine in New York. He watched ambulances collect heart attack victims from his neighborhood. He returned to Sankyo Pharmaceutical Company in Tokyo with a hypothesis: fungi competing for resources in soil would evolve inhibitors of the same cholesterol synthesis enzyme that causes heart disease in humans — because the pathway is conserved across living organisms and poisoning a competitor’s sterol synthesis is a viable survival strategy.
Endo was deliberately searching fungi for HMG-CoA reductase inhibitors. HMG-CoA reductase is the enzyme that controls the rate limiting step in the liver’s cholesterol synthesis pathway. He screened approximately 6,000 fungal cultures over two years. In 1973, he found what he was looking for in Penicillium citrinum — a mold from a grain shop in Kyoto.
The compound he isolated inhibited HMG-CoA reductase with an affinity approximately 10,000 times greater than the natural substrate. The molecule that eventually became lovastatin (Mevacor) was purified from Aspergillus terreus and received FDA approval in 1987.
What makes the biosynthetic detail so interesting: Aspergillus terreus carries, in its own genome, a drug resistant copy of the very enzyme its metabolite inhibits. The producing organism evolved the poison and the antidote simultaneously — confirming exactly what Endo predicted. Fungi produce HMG-CoA reductase inhibitors as competitive weapons. We isolated, purified and packaged that weapon as a pill to help lower cholesterol.
An aside I’d like to add; I disagree with the currently held medical opinion of cholesterol as an enemy, but this article isn’t about that.
“Low total cholesterol is associated with higher all cause mortality, often exhibiting a U-shaped or J-shaped risk curve where both very low and high levels increase risk. While extremely high cholesterol correlates with cardiovascular death, low cholesterol is strongly linked to higher mortality.”
But the important question the statin story asks, but mainstream medicine has neither answered nor seemingly considered is this: if a cardiologist’s patient is being prescribed a fungal metabolite specifically because it inhibits cholesterol synthesis and therefore lowers cholesterol predictably, why is it a leap to consider that a patient who has been living in a water damaged home with mycotoxin producing organisms — and who presents with anomalously low cholesterol — may be receiving the same biochemical intervention, only through environmental rather than pharmaceutical means? If the mechanism is real enough to anchor a $16 billion drug market, it is real enough to investigate as an exposure route.
Why is the inhalational and transdermal absorption pathway through building exposure considered categorically implausible when the oral pharmaceutical pathway is not only plausible but standard of care?
Holistic health and home consultants: how many times have you seen dangerously low cholesterol in your mold patients’ labs? In my own experience, I had a total cholesterol of 120 mg/dL when I was in my sick townhouse.
Mycophenolate: A Potent Immunosuppressant
Mycophenolic acid, which you may recognize if you’ve ever taken a urine mycotoxin test, has a stranger history than statins but again comes from fungi.
In 1893, 35 years before Fleming discovered penicillin, an Italian physician named Bartolomeo Gosio isolated a crystalline compound from Penicillium glaucum and demonstrated it inhibited the growth of anthrax. It was the first antibiotic ever isolated in pure crystalline form. (However, it was not clinically adopted as an antibiotic due to its toxicity.)
The compound was re-isolated, renamed and recharacterized multiple times over the next century before Syntex Research finally had an application for it. Mycophenolate mofetil (CellCept) received FDA approval in 1995 for prevention of organ transplant rejection. It is now the 227th most prescribed drug in the United States. While both mycophenolate and cyclosporine, referenced above, are used as anti-rejection drugs, they have different mechanisms of action.
Mycophenolic acid inhibits inosine-5’-monophosphate dehydrogenase (IMPDH), the rate limiting enzyme in the de novo synthesis of guanosine nucleotides and purine synthesis. T and B lymphocytes cannot compensate for this blockade the way most other cells can, they depend on the pathway too heavily during proliferation. The result is selective suppression of the adaptive immune response. The molecule’s entire clinical purpose is to stop the immune system from functioning normally, preventing it from recognizing and rejecting a foreign organ or tissue.
It comes from a Penicillium species. Penicillium brevicompactum is among the five most common Penicillium species found in indoor environments and is even measured on ERMI (see my ERMI breakdown post here).
How many people in water damaged buildings report immune system disturbance or an underactive immune response, with recurrent illness as a common hallmark?
A 2017 study published in Applied and Environmental Microbiology demonstrated that P. brevicompactum growing on wallpaper produced mycophenolic acid at levels of 1.8 mg per square meter and that 15% of it became airborne at air velocities as low as 0.3 meters per second. That is approximately the speed of air displaced by a person walking through a room. Mycophenolic acid was distributed across multiple particle size fractions including particles small enough to penetrate deep into the respiratory tract.
A Finnish pilot study published in 2022, small by design, with urinary analysis conducted on two occupants, detected mycophenolic acid in both workers’ urine from the same water damaged office building. Neither was taking immunosuppressive drugs.
The question posed in the study: was the detected mycophenolic acid in the workers’ urine evidence of exposure in the building? Naturally, the conclusion of the paper was… more studies were needed.
The Problem With Measuring Something You Can’t See
The obstacles to proving indoor mycotoxin exposure are not one problem. They are many, layered on top of each other in ways that make the question extraordinarily difficult to answer with the tools currently being applied.
Obstacle One: Standard indoor testing measures the organism, not what it produces
Standard indoor air quality testing uses spore trap sampling — a device pulls 75 to 150 liters of air through a cassette, a lab looks at the cassette under a microscope and counts spores. This is what most mold inspections report in their findings. There is also surface sampling — tape lift or swab — but these have the same limitation because they are read the same way, via microscopy, and similarly only the organism is reported on.
But spores are the organism. Mycotoxins are what the organism produces; secondary metabolites, chemical compounds that travel through air on an entirely different type of particle. They are also odorless, colorless and have no visual signature whatsoever. A test that counts spores is not a test for mycotoxins. These are not the same measurement.
Obstacle Two: Mycotoxins travel on particles standard air tests cannot capture
Fungal spores are relatively large particles (relative to metabolites) typically 2 to 30 microns in diameter. Air testing equipment is designed to capture these. Mycotoxins, however, do not always travel attached to spores. They travel on hyphal fragments — microscopic pieces of fungal structure — and on submicron particles far smaller than any spore.
Research published in Applied and Environmental Microbiology found that these fungal fragments are released into air in numbers up to 320 times higher than spores and that fragment counts bear no predictable relationship to spore counts. A separate study examined Stachybotrys chartarum — the species commonly referred to as “black mold” — using air filters designed to capture only particles smaller than one micron in diameter. Spores, which are larger than one micron, were completely excluded from these filters. The filters still contained measurable trichothecene mycotoxins. The spore test read clean of course. The mycotoxins were in the air on particles the test was never designed to detect.
Proving mycotoxins are in the air is a crux of many legal arguments regarding building exposure and the risks and liability of it.
Obstacle Three: single point air sampling misses sources that aren’t in the room
Even assuming air testing is a highly accurate method for detecting spores in a built environment (it’s not), you are still only looking for one thing usually in one area. Air dynamics, HVAC cycling, foot traffic and door movement all influence what is airborne at any given moment. A snapshot taken at one location, at one time, in a building with hidden contamination tells you very little about chronic inhalation exposure.
Obstacle Four: Better tests exist but face a catch-22
Dust sampling — which measures accumulated mycotoxin content on settled surfaces over time using LC-MS/MS or ELISA methodology — can be a more meaningful proxy for chronic environmental load. Laboratories can confirm the presence of specific mycotoxins in a home using the same analytical technology the FDA uses to regulate food. But critics argue that confirmation of mycotoxins in environmental dust does not prove they were or are airborne and thus the route of exposure is called into question. Yet the same people making this argument accept that a pharmaceutical compound derived from these same organisms, administered orally at milligram doses, produces systemic immunosuppression, cholesterol synthesis disruption or antibiotic effects…
A mold colony the size of a dinner plate, growing in a wall cavity, is producing these compounds often daily. (You need certain conditions for both fungal growth and secondary metabolite generation from a colony.) Those compounds accumulate in settled dust. They aerosolize on submicron particles with normal air movement. And yet the standard of evidence required to establish harm is so high and the testing methodology so misaligned with the actual compounds in question that the question effectively cannot be answered with currently accepted tools. That is not a scientific conclusion. It is a measurement problem being mistaken for one.
Obstacle Five: Building air dynamics are variable by design
Every building, depending on its assembly, occupants and heating and cooling systems, is different. Air volumes vary significantly. Consider a home with 15 foot cathedral ceilings versus a traditional Cape Cod style home with 9 foot ceilings. Air currents differ between a home with forced air HVAC and one that relies on window units and baseboards. Standardized sampling protocols applied to environments this varied in their physical characteristics will produce results that are difficult to compare and even more difficult to interpret as a reliable measure of chronic personal exposure.
Obstacle Six: Measurement in toxicology only means something when a threshold exists
In toxicology, a detected concentration of a toxicant only becomes clinically meaningful when there is an established threshold at which harm occurs. As you will see below, such thresholds exist for mycotoxins in food but none exist for mycotoxins in the built environment, or mold spores for that matter. Without an established limit for the organism itself, there is no framework for establishing a limit for its secondary metabolites, which means even accurate detection cannot be formally characterized as dangerous by current standards.
What Doctors Were Never Taught
No standardized US medical school curriculum covers mycotoxicosis from indoor environmental exposure. This is not a criticism of physicians. It is a reality about how medical bodies train doctors. Even within environmental medicine subspecialties, mycotoxicosis receives, at most, a single textbook chapter dedicated to its existence and is only mentioned in the context of occupational hazard — grain workers, agricultural settings, food processing facilities etc.
The ICD-10 coding structure, that dictates insurance billing, reflects this gap directly and is worth understanding in some detail because, in the American health system, a reimbursement code is the baseline unit of clinical recognition. Without a code, there is no billing. Without billing, there is no clinical pattern to study. Without clinical data, there is no real research pathway.
ICD-10 code T64 — “Toxic effect of aflatoxin and other mycotoxin food contaminants” — specifically frames mycotoxin exposure as a food contamination event. There is no code for inhalational exposure in a residential setting.
A separate code, Z77.120 — “Contact with and (suspected) exposure to mold (toxic)” — does exist and has been billable since 2016. But it is a contextual exposure code, not a diagnosis code. It documents that a patient may have been in contact with toxic mold. It does not specify route of exposure, duration, concentration or mechanism of harm. It does not distinguish between a patient who briefly entered a moldy basement and one who has been sleeping next to a hidden Stachybotrys colony for eighteen months. A 2024 study examining insurance claims data found that when Z77.120 is used, the associated diagnoses are predominantly upper respiratory — allergic rhinitis, asthma, acute upper respiratory infection. The systemic picture — immune dysregulation, neurological symptoms, metabolic disruption — is not captured. The study’s own authors noted the code description is “somewhat ambiguous” and likely reflects patient reported exposure, with the biologically relevant parameters (location, duration, concentration) entirely unknown.
Most physicians still do not know either code exists.
Perhaps you recently saw the controversy and backlash on Instagram regarding the American Academy of Allergy, Asthma & Immunology (AAAAI), who posted on Instagram claiming “MYTH: TOXIC MOLD EXPOSURE CAUSES A WIDE RANGE OF SYMPTOMS LIKE FATIGUE, HEADACHE AND BRAIN FOG.” There was such a public outcry that the organization took the post down and backtracked on (not retracted) their position. Their official position however, still exists on their website in an article titled “Toxic Mold Syndrome: Separating Fact from Fiction” — linked here. That article actually highlights the core issues I have highlighted in this article and previously as reasons why mold toxicity isn’t clinically validated. It’s interesting their opinion lands on the opposite side of the spectrum with the available data especially since they state the following:
“There is a clear, well established relation between damp indoor spaces and detrimental health effects. Unfortunately, the mechanism(s) driving the effects remains uncertain or controversial. Further, engineering science is still not able to clearly define what a ‘damp building’ is. There is currently no universally accepted standard for safe levels of mold in indoor environments.”
So the physician who prescribes lovastatin — a molecule derived from Aspergillus terreus to inhibit HMG-CoA reductase — was never taught that it came from a mold. Pharmacology training largely covers mechanism of action. It does not cover origin. If it did, the conversation a prescribing cardiologist has with a patient reporting cholesterol irregularities after two years in a water damaged home might look different — though it would still require a curious physician willing to make the connection and one who doesn’t believe “the lower the cholesterol the better.”
The American College of Occupational and Environmental Medicine produced a 2002 position statement concluding that indoor mycotoxin exposure had not been proven harmful. A published critique later documented that the lead authors had undisclosed financial relationships with the insurance defense industry. The American College of Medical Toxicology’s current guidance acknowledges that “traditional medical training often does not cover these conditions extensively.” George Washington University School of Medicine offers a continuing medical education course on mold illness, which is a step in the right direction, but continuing education is not curriculum. (Headed by Dr. Andrew Heyman who worked alongside Dr. Shoemaker for many years and helped expand CIRS treatment.)
The most comprehensive mainstream assessment — the National Academy of Medicine’s 2004 report “Damp Indoor Spaces and Health” — found sufficient evidence associating dampness and mold with upper respiratory symptoms, wheezing and asthma exacerbation, again focusing on respiratory symptoms only and neglecting systemic effects. A Lawrence Berkeley National Laboratory meta-analysis found a 30 to 50 percent increase in respiratory and asthma related health outcomes in occupants of damp buildings. The WHO guidelines on dampness and mold acknowledge sufficient epidemiological evidence for increased risk of respiratory illness. None of this has translated into clinical training, diagnostic criteria or reimbursable codes. Reimbursement codes keep being reiterated here because sadly, especially in the American health system, that is the baseline for clinical recognition and even with the newer codes referenced above, most physicians still don’t know they exist.
The Government Knows Mycotoxins Harm at Low Doses
There is an underappreciated irony embedded in US food safety regulations that for some reason, never translates to the bedside.
The FDA sets an action level of 20 ppb for total aflatoxins in human food — the concentration at which the government considers corn, peanuts and other commodities too contaminated for sale. The EU sets its limit at 4 ppb for the same foods. For baby food, the EU limit is 0.1 ppb — effectively 200 times stricter than the general US threshold. No surprise there since American regulations generally set higher limits or allow for things the EU has banned or severely limited for decades. The FDA sets a guidance level for fumonisins at 2 to 4 ppm in corn products, an advisory level for deoxynivalenol (DON) at 1 ppm in finished wheat products, and a limit of 50 ppb for patulin in apple juice.
These are not arbitrary numbers. They are risk management thresholds derived from dose response data acknowledging that these compounds cause harm — at low concentrations, through ingestion, over time. IARC classifies aflatoxin B1 as a Group 1 carcinogen. JECFA (WHO) refuses to establish a tolerable daily intake for aflatoxins because they are genotoxic with no safe lower threshold.
A 2018 FDA survey found one or more mycotoxins in 69% of infant and toddler foods tested in the US retail market.
The government monitors mycotoxins in food using the same LC-MS/MS technology that can detect them in homes. It sets limits because it accepts the dose-response relationship as real. The logic that applies to a contaminated corn crop does not, apparently, apply to a contaminated building — even when occupants spend 16 to 24 hours a day inside it.
Strangely, the argument many physicians use to discount urinary mycotoxin test results relies on precisely this regulatory knowledge: that allowable mycotoxin levels exist in food**,** and that cumulative dietary exposure from multiple contaminated foods eaten multiple times a day could explain elevated urinary readings. The conclusion drawn is that food must be the sole source. The building, apparently, does not count.
Despite all of this, there is still no threshold or regulatory limit for mold organism load in a building deemed “toxic” or unacceptable. Without that, how could we possibly have a quantifiable danger threshold for its secondary metabolites?
Now, exposure route DOES matter. If you are bitten by a venomous snake you can get very sick. If you swallow the same venom though you do not get the same response. Bloodstream vs. ingestion is different. Different toxins are more toxic through certain routes of entry and lower or non toxic in others. But we have proof ingestion of mycotoxins is metrically bad and we also have proof that mycotoxins can be absorbed transdermally (through the skin) and go into systemic circulation through inhalation but the government seemingly isn’t interested in determining if those 2 routes have similar effects as ingestion and may need further investigation to set threshold limits.
Oh wait…. (see below)
Weaponization of Mycotoxins
There is perhaps no more clarifying data point in this entire conversation than this: mycotoxins have been recognized and used as biowarfare.
In 1995, the government of Saddam Hussein admitted to United Nations weapons inspectors that its scientists had weaponized aflatoxin, a mycotoxin produced by Aspergillus species, the same genus that often exists in water damaged buildings. Iraq admitted to UNSCOM that it had produced 2,200 liters of aflatoxin and prepared aflatoxin filled warheads and aerial bombs. According to UNSCOM’s deputy executive chairman Charles Duelfer, aflatoxin has no conventional battlefield use, it causes liver cancer. Its intended purpose was long term, insidious harm. Richard Spertzel, the chief biological weapons inspector for UNSCOM, called it “the cruelest weapon — it means watching children die slowly of liver cancer.” Global Security + 2
The trichothecene mycotoxins have a parallel history. During the 1970s and 1980s, trichothecene mycotoxins gained notoriety as biological warfare agents implicated in “Yellow Rain” attacks in Southeast Asia. T-2 mycotoxin is highly toxic and, notably, is the only mycotoxin studied to be effective through transdermal exposure as well as inhalation and ingestion. Because of its antipersonnel properties, ease of large scale production and delivery via aerial dispersal, it has been described as having “excellent potential for weaponization.” In 1982, US Secretary of State Alexander Haig and his successor George Shultz formally accused the Soviet Union of using T-2 mycotoxin as a chemical weapon in Laos, Cambodia and Afghanistan, allegedly causing thousands of casualties. The scientific debate over Yellow Rain remains contested — a countertheory attributed the yellow substance to mass bee defecation, and the evidence was disputed (lol) — but the point that matters here is not which side prevailed. The point is that US government and academic laboratories tested environmental and biomedical samples linked to Yellow Rain reports, and findings of trichothecene markers were publicly cited as evidence of deliberate toxin use. The US government treated trichothecene mycotoxin exposure as a matter of national security, commissioned laboratory analysis and brought the allegation before Congress and the international community. nih + 2
The CDC currently classifies trichothecene mycotoxins as Category B potential bioterrorism agents — the same classification as Q fever, brucellosis and viral encephalitis.
The same class of mycotoxins that the US government alleged were used as a weapon against civilian populations — the same compounds that Iraq filled into warheads — are produced naturally by mold species commonly found in water damaged homes. The US government did not, in those contexts, argue that inhalational and dermal mycotoxin exposure was biologically implausible. It argued the opposite, with enough conviction to raise it on the floor of Congress and before the UN Security Council. And yet when a patient walks into an exam room and reports living in a building with documented Stachybotrys or Aspergillus contamination, the same federal infrastructure that classified these compounds as weapons grade threats somehow cannot extend that logic to a residential exposure route.
The compounds are the same. The organisms producing them are the same. The routes of exposure — inhalation, dermal contact, ingestion — are the same ones the military considered sufficient to cause mass casualties. The dose is different. But the question of whether chronic low level exposure to a weaponized class of compounds produces subclinical biological effects has never been seriously asked in a residential context. It has only been avoided.
Access to These Metabolites Indicates a Known Truth…
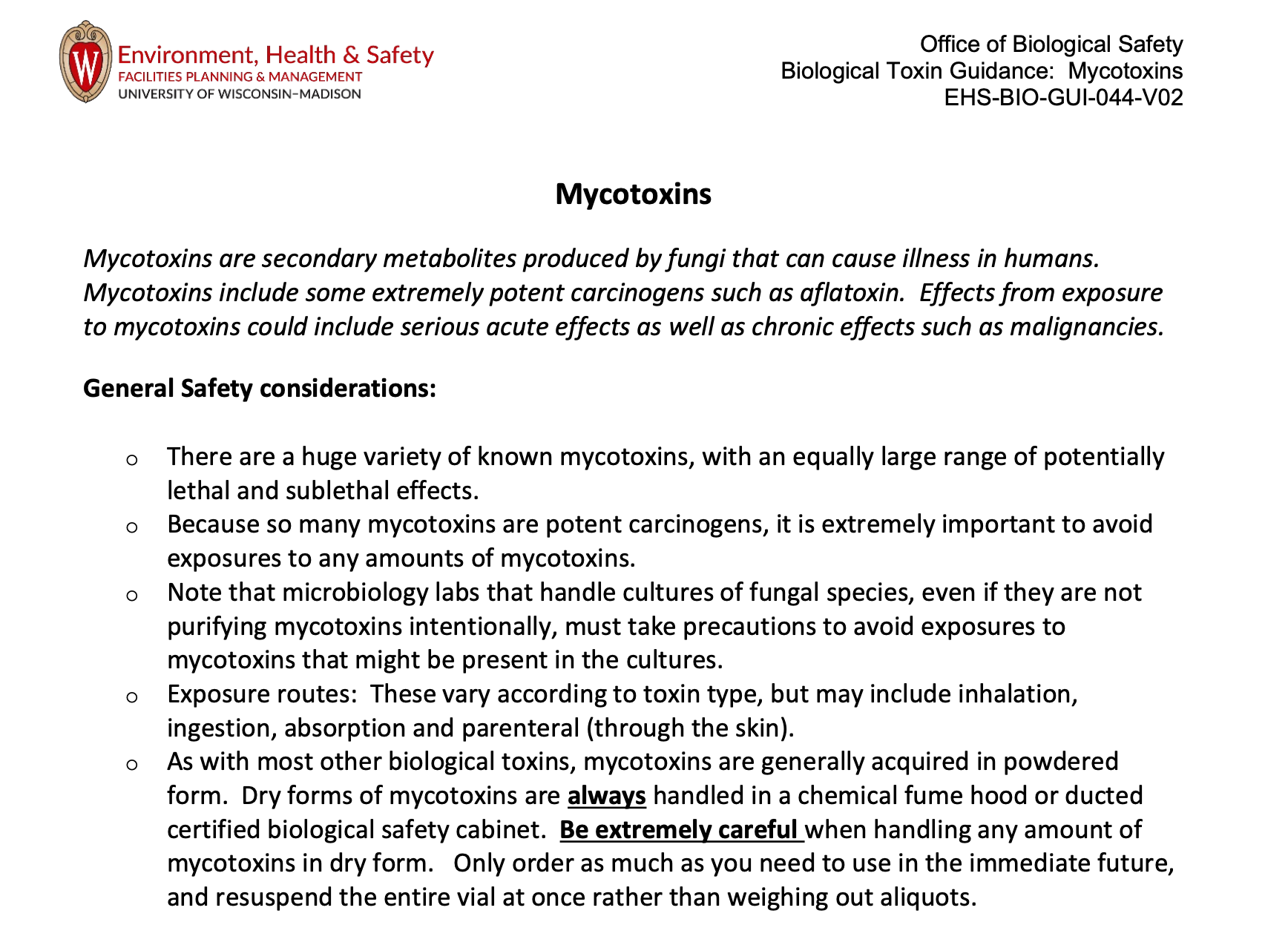
One final detail worth knowing. In the United States, mycotoxins cannot be handled in a standard laboratory setting. Biotoxins with an LD50 less than 50 mg/kg — a category that includes aflatoxin and other mycotoxins — are classified as risk group 2 biotoxins requiring Biosafety Level 2 containment. This is not a suggestion. It is a regulatory requirement. Risk Assessment Biosafety Level
More revealing still: that BSL 2 threshold applies to the chemical compound itself. The moment you aerosolize it — the moment you introduce it into air in a way that permits inhalation exposure — the requirement elevates. BSL 3 or higher is mandated for work with aerosolized mycotoxins.
This is institutional acknowledgment, codified in safety guidance, that aerosolized mycotoxins are sufficiently hazardous to warrant the highest level of containment available in research settings. The government does not regulate things lightly. It does not require BSL 3 containment for harmless compounds. It requires it for materials that, when suspended in air and inhaled, pose a serious threat to human health.
Will Medicine Ever Accept the Fungal Facts?
Ochratoxin A, produced by several Aspergillus and Penicillium species common to both food and indoor environments, has a 35-day half life in human plasma. It is 99.8% bound to serum albumin. It does not clear readily. It bioaccumulates.
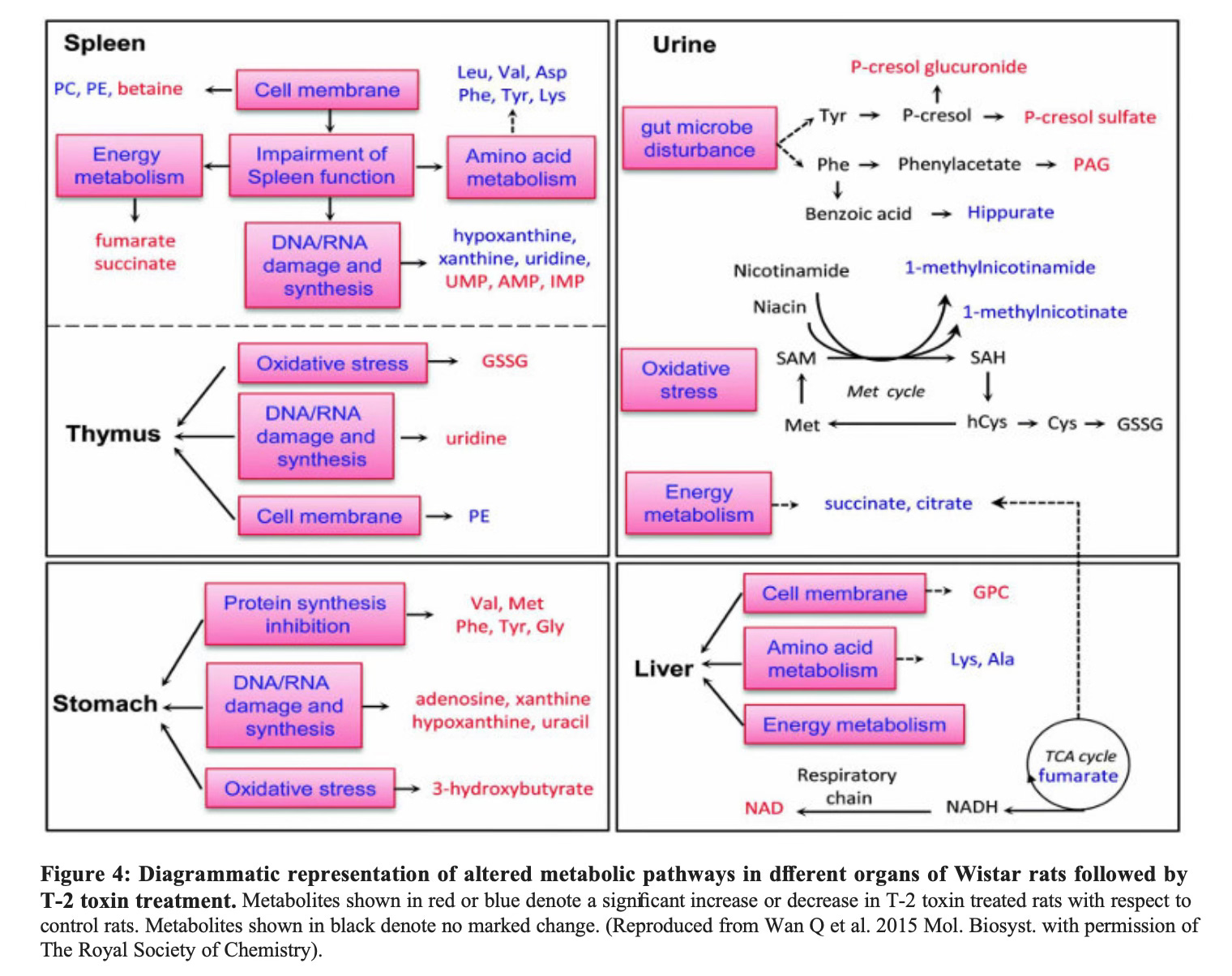
Mycophenolic acid from P. brevicompactum has been found in the urine of building occupants. Gliotoxin from Aspergillus fumigatus, a ubiquitous indoor species, induces monocyte apoptosis and suppresses antigen presentation at concentrations below those found in patients with invasive aspergillosis. T-2 toxin causes thymic atrophy and leukopenia. Deoxynivalenol inhibits human lymphocyte proliferation by 50% at concentrations far below those causing acute symptoms.
These are not obscure findings. They are in the peer reviewed literature, published in journals like Blood, Applied and Environmental Microbiology, Toxins, The Royal Society of Chemistry and the International Journal of Molecular Sciences.
The question is not whether these compounds are biologically active. Medicine has answered that question… and built a $50 billion annual industry on the answer. The question is whether the same activity occurs when exposure happens through inhalation of submicron particles in a confined space, at chronic low dose concentrations, over months or years rather than in a single controlled dose. The word “lower” deserves scrutiny. A bioaccumulating compound with a 35 day half life in a person living in a contaminated environment may not represent lower exposure in any meaningful cumulative sense.
That question has not been seriously resourced or if it has, has not been readily shared and dispersed. It has not been systematically studied in humans. And here is the kicker: we don’t have studies that can answer it because it is be considered unethical to intentionally expose people to a known toxin. Read that again.
The research that would answer it has not been funded and seemingly has no plans to be and when you think about what the government, building and insurance industries have to lose if we get the expected answers and set toxicity thresholds, it starts to make sense why…
And so patients continue to arrive in exam rooms. With cholesterol panels that don’t make sense for their age, diet, lifestyle or genetics, with immune systems erroneously attacking things they shouldn’t be or not responding at all (autoimmunity), with brain fog, with fatigue that doesn’t respond to more sleep, with unexplainable and rare cancer, with symptoms their doctors cannot explain — after living in buildings that contain, in their walls, their ducts and their settled dust, the same class of organisms and compounds that gave us the drugs those same doctors prescribe.
The mechanism is not a mystery. It is in the pharmacology textbooks.
This article draws on published literature across pharmacology, environmental microbiology, toxicology and food safety science. Sources include research from PubMed Central, the FDA, the National Academy of Medicine, the WHO, the Lawrence Berkeley National Laboratory and peer reviewed journals including Applied and Environmental Microbiology, Toxins, Blood and the American Scientist.
Where Your Home Meets Your Health — The Guided Well
Sources:
Statins and fungal origin
Endo A. “The discovery and development of HMG-CoA reductase inhibitors.” Journal of Lipid Research.1992;33(11):1569–82.
Endo A, Kuroda M, Tsujita Y. “ML-236A, ML-236B, and ML-236C, new inhibitors of cholesterogenesis produced by Penicillium citrinum.” Journal of Antibiotics. 1976;29(12):1346–8.
Tobert JA. “Lovastatin and beyond: the history of the HMG-CoA reductase inhibitors.” Nature Reviews Drug Discovery. 2003;2(7):517–26.
Kennedy J, et al. “Modulation of polyketide synthase activity by accessory proteins during lovastatin biosynthesis.” Science. 1999;284(5418):1368–72. PMID 10334994.
Reider A, et al. “From Fleming to Endo: The discovery of statins.” PMC9491398. 2022.
Akira Endo obituary. The Lancet. 2024. PMID: PIIS0140-6736(24)01497-1.
Statins — market and mechanism
HMG-CoA Reductase Inhibitors. StatPearls. NCBI Bookshelf. NBK542212.
Data Bridge Market Research. Global Statin Market Report. 2024.
Mycophenolate and mycophenolic acid
Bentley R. “Mycophenolic acid: a one hundred year odyssey from antibiotic to immunosuppressant.” Chemical Reviews. 2000;100(10):3801–26. PMID 11854616.
Allison AC, Eugui EM. “Mycophenolate mofetil and its mechanisms of action.” Immunopharmacology.2000;47(2–3):85–118. PMID 10878285.
FDA CellCept Approval History. Drugs.com.
Penicillin and Fleming
Fleming A. “On the antibacterial action of cultures of a Penicillium, with special reference to their use in the isolation of B. influenzæ.” British Journal of Experimental Pathology. 1929;10(3):226–236.
van Boeckel T, et al. “Alexander Fleming (1881–1955): Discoverer of penicillin.” PMC4520913.
Cyclosporine
Borel JF, et al. “Biological effects of cyclosporin A: a new antilymphocytic agent.” Agents and Actions.1976;6(4):468–75.
FDA approval history, cyclosporine (Sandimmune), 1983.
Fingolimod / myriocin
Graler MH, Goetzl EJ. “Fingolimod (FTY720): a recently approved multiple sclerosis drug based on a fungal secondary metabolite.” PubMed PMID 21456524.
Ergot alkaloids
Tudzynski P, et al. “Biosynthetic Pathways of Ergot Alkaloids.” PMC4280535.
Hofmann A. LSD: My Problem Child. McGraw-Hill, 1980.
Fungal drug discovery — comprehensive surveys
Prescott TAK, et al. “Fungal Drug Discovery for Chronic Disease: History, New Discoveries and New Approaches.” PMC10296638. 2023.
Kealey T, et al. “Bioactive Products from Fungi.” PMC7122484. 2020.
Kew Royal Botanic Gardens. “The fungal drug discovery revolution.” kew.org.
Mycotoxin aerosolization and indoor air
Aleksic B, et al. “Aerosolization of Mycotoxins after Growth of Toxinogenic Fungi on Wallpaper.” Applied and Environmental Microbiology. 2017;83(16). PMC5541226.
Brasel TL, et al. “Detection of Airborne Stachybotrys chartarum Macrocyclic Trichothecene Mycotoxins on Particulates Smaller than Conidia.” Applied and Environmental Microbiology. 2005;71(1):114–122. PMC544211.
Górny RL, et al. “Fungal Fragments as Indoor Air Biocontaminants.” Applied and Environmental Microbiology.2002;68(7):3522–31. PMC126767.
Adhikari A, et al. “Fungal Fragments in Moldy Houses: A Field Study in Homes in New Orleans and Southern Ohio.” PMC2153459. 2009.
Finnish pilot study — urinary MPA detection
Vaali K, Tuomela M, Mannerström M, Heinonen T, Tuuminen T. “Toxic Indoor Air Is a Potential Risk of Causing Immuno Suppression and Morbidity — A Pilot Study.” Journal of Fungi. 2022;8(2):104. PMC8877819. DOI: 10.3390/jof8020104.
Ochratoxin A and immune effects
Studer-Rohr I, et al. “The occurrence of ochratoxin A in coffee.” Archives of Toxicology. 2000;74(8–9):499–510.
Systematic review: “Effect of Ochratoxin A (OTA) on the Immune System.” Toxins. 2025;17(5):256. PMC12115609.
Gliotoxin and Aspergillus immune suppression
Stanzani M, et al. “Aspergillus fumigatus suppresses the human cellular immune response via gliotoxin-mediated apoptosis of monocytes.” Blood. 2005;105(6):2258–65. PMID 15546954.
Trichothecenes and immune effects
Agriopoulou S, et al. “T-2 Toxin — The Most Toxic Trichothecene Mycotoxin: Metabolism, Toxicity, and Decontamination Strategies.” MDPI Molecules. 2021;26(22):6868.
Pestka JJ, et al. “Deoxynivalenol-induced immunomodulation of human lymphocyte proliferation and cytokine production.” Food and Chemical Toxicology. 2001. PMID 11434990.
Mold, mycotoxins and immune dysregulation
Kraft S, Buchenauer L, Rinne T. “Mold, Mycotoxins and a Dysregulated Immune System: A Combination of Concern?” International Journal of Molecular Sciences. 2021;22(22):12269. PMC8619365.
FDA food mycotoxin regulations
FDA. “Mycotoxins.” fda.gov/food/natural-toxins-food/mycotoxins.
FDA Compliance Policy Guide Sec. 555.400 — Aflatoxins in food.
FDA Guidance for Industry: Fumonisin Levels in Human Foods and Animal Feeds. November 2001.
FDA Guidance: Advisory Levels for Deoxynivalenol (DON). June 2010.
Zhang Y, et al. “Mycotoxins in infant/toddler foods and breakfast cereals in the US retail market.” Food Additives and Contaminants. 2018. PMID 29575988.
Weaponized Mycotoxins
https://www.ebsco.com/research-starters/chemistry/mycotoxins-biological-weapons
ERMI and dust based testing
Vesper S, et al. “Higher Environmental Relative Moldiness Index (ERMI) Values Measured in Homes of Asthmatic Children.” PMC3874819. 2013.
ICD-10 coding
ICD-10-CM T64: Toxic effect of aflatoxin and other mycotoxin food contaminants. icd10data.com.
ICD-10-CM Z77.120: Contact with and (suspected) exposure to mold (toxic). Effective FY2016. icd10data.com.
Kanu F, et al. “Healthcare use and health disparities associated with mold exposure diagnosis codes.” PMC11162893. 2024.
Medical education and institutional position statements
Institute of Medicine. Damp Indoor Spaces and Health. National Academies Press, 2004. DOI: 10.17226/11011.
WHO. Guidelines for Indoor Air Quality: Dampness and Mould. 2009.
Fisk WJ, Lei-Gomez Q, Mendell MJ. “Meta-analyses of the associations of respiratory health effects with dampness and mold in homes.” Indoor Air. 2007;17(4):284–96. PMID 17661925.
Critique of ACOEM statement: PMID 19043916.
GWU School of Medicine CME: “Understanding Mold Illness: The Basics.” cme.smhs.gwu.edu.
American Scientist source article
“Statins: From Fungus to Pharma.” American Scientist. americanscientist.org/article/statins-from-fungus-to-pharma